The Art of Rhinoplasty
Dr. Rafizadeh, a board certified plastic surgeon in NJ, has been one of New Jersey's most prominent rhinoplasty specialists for over 30 years. He is mindful of both what the patient wants to achieve and what is safely achievable — and he is always baffled when he sees someone send a photo showing only the nose, without considering the rest of the face.
The nose is an integral part of the face. Any change in the shape of the nose must relate to the surrounding features — the chin, the upper lip philtrum, the width of the face. A tip that appears wide in a narrow face might look perfectly acceptable in a wider face. Dr. Rafizadeh evaluates the nose in complete harmony with the full facial structure before recommending any change.
“The rhinoplasty procedure is one of the most interesting and challenging in plastic surgery. It takes experience, precision, and artistry to achieve great results — and respect for the structures of the nose, especially the tip cartilages, is essential for long-term success.”

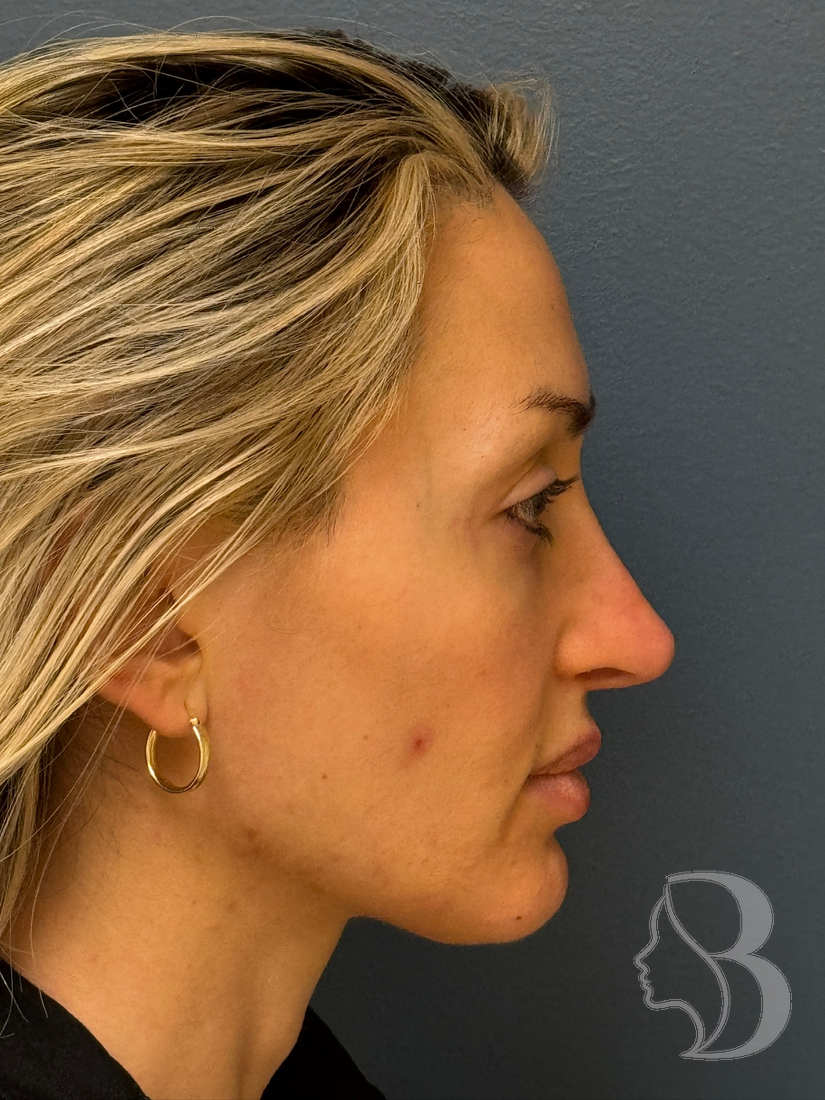
Rhinoplasty Before & After
View Full Gallery →








Open vs. Closed Rhinoplasty
Dr. Rafizadeh conceptually divides the nose into an upper bony part and a lower cartilaginous part. He selects either an open rhinoplasty (with a small incision across the columella for maximum visibility) or a closed rhinoplasty (with all incisions inside the nostrils, leaving no visible scars) based on the complexity of correction required and each patient's anatomy.
What Can Rhinoplasty Address?
Common concerns Dr. Rafizadeh addresses include: dorsal humps or bumps on the bridge, a wide or bulbous nasal tip, asymmetry, a drooping or upturned tip, wide nostrils, a deviated septum affecting breathing, and overall disproportion to the rest of the face. Secondary (revision) rhinoplasty for patients dissatisfied with prior surgeries is also performed.
Submental Liposuction
Dr. Rafizadeh often combines rhinoplasty with submental liposuction — removing a small amount of fat under the chin — when appropriate. This combination establishes balance and harmony across the profile in a way that rhinoplasty alone cannot always achieve. A chin implant is also occasionally added to improve the chin-nose relationship on profile view, and a lip lift may be considered when the philtrum length and tooth show are part of the aesthetic plan.
Recovery & Timeline
How Dr. Rafizadeh Approaches the Nose
The nose is an integral part of the face — any change in its shape must relate to the rest of the face. The tip that looks wide in a narrow face could look perfectly acceptable in a wider face. On the profile view, the chin and nose relate closely; the upper lip philtrum height relates to the nose as well. The technical aspects of rhinoplasty are well understood, but the artistic understanding of how the nose relates to the rest of the face is far less appreciated.
Dr. Rafizadeh divides the nose into an upper bony part and a lower cartilaginous part. The bone forms an arch making the nasal bridge; below this the upper lateral cartilages continue that arch. The shape of the tip is determined by the lower lateral cartilages — a pair shaped like an inverted U. He has particular respect for these tip cartilages, since careful handling is key for long-term results.
Functional Rhinoplasty & the Airway
When the septum deviates and the turbinates are enlarged, breathing becomes difficult. In many patients — especially those with a previous rhinoplasty — the lower lateral cartilages collapse against the septum, obstructing the airway. Dr. Rafizadeh takes a reconstructive approach, placing spreader grafts to open this area, improving both breathing and the pinching appearance above the tip simultaneously. When a dorsal hump is removed and the nasal bones are brought together, the lower half of the nose needs internal support — without it the upper lateral cartilages can collapse, creating an internal valve obstruction. Spreader grafts made from harvested septal cartilage prevent this collapse.
Computer Imaging & the Consultation
Dr. Rafizadeh uses computer imaging to show patients exactly what he has in mind and confirm alignment before surgery. A typical rhinoplasty involves reducing the dorsal hump, bringing the nasal bones together to recreate the arch, and in many cases refining the tip. The best long-term results are achieved when the tip is left unmodified unless necessary. After surgery, a splint is worn for one week. Ninety-five percent of swelling resolves within a month; the final 5 percent can take six months to one year.
Rhinoplasty in New Jersey
Dr. Rafizadeh has performed rhinoplasty in New Jersey for over 30 years, making him one of the most experienced nose surgeons in the state. Patients travel from throughout New Jersey — Morristown, Short Hills, Summit, Chatham, Westfield, Princeton, and across Morris, Essex, Somerset, and Union counties — as well as from New York City and beyond. Common concerns include dorsal humps, wide or bulbous nasal tips, and breathing problems from a deviated septum or collapsed nasal valves.
Patients comparing rhinoplasty doctors in NJ should weigh more than proximity. The nose is the most technically unforgiving operation in plastic surgery, so the surgeon's depth of rhinoplasty experience, board certification by the American Board of Plastic Surgery, and a portfolio of natural before-and-after results matter far more than any single credential or marketing claim. Among rhinoplasty doctors in New Jersey, Dr. Rafizadeh stands out for treating the nose as part of the whole face, for handling primary, functional, revision, and ethnic cases under one roof, and for using computer imaging so every patient sees and agrees on the plan before surgery. For a deeper look at specific rhinoplasty topics, see Dr. Rafizadeh's articles on dorsal hump rhinoplasty, hanging columella correction, and nasal collapse after rhinoplasty.
→ Schedule a ConsultationMeet with Dr. Rafizadeh personally to discuss your goals and a personalized plan. Call (973) 267-0928 or request a consultation online.Top Rhinoplasty Doctors in New Jersey
When patients search for the top rhinoplasty doctors in New Jersey, they often find a mix of ENT and facial-plastics specialists. What sets Dr. Rafizadeh apart among the best rhinoplasty surgeons in NJ is a full plastic-surgery perspective: he plans every nose in proportion with the brow, eyes, chin, lip, and overall facial frame, rather than in isolation. That whole-face judgment is what separates a result that simply removes a hump from one that genuinely improves the face.
Use a short, honest checklist to compare any of the rhinoplasty doctors in NJ you are considering: board certification by the American Board of Plastic Surgery, a high annual volume of nose surgery, before-and-after galleries showing noses and skin types like yours, comfort with both open and closed technique, a clear plan to protect your breathing, and a real revision policy. Dr. Rafizadeh meets each of these — ABPS board certified, ACS Fellow (FACS), more than 30 years of rhinoplasty in Morristown, and experience spanning primary, functional, revision, and ethnic cases — which is why patients across northern and central New Jersey and the greater New York area choose his practice for nose surgery.
Rhinoplasty Techniques
Not every rhinoplasty is the same operation. Dr. Rafizadeh selects the approach that best fits each patient's anatomy, degree of correction required, and long-term structural goals. Understanding the options helps you arrive at your consultation with the right questions.
Preservation Rhinoplasty
Preservation rhinoplasty represents the most significant technical advance in rhinoplasty in the last two decades. Rather than removing cartilage and bone to reshape the nose, preservation technique keeps the native dorsum intact and repositions it — either via a push-down or let-down maneuver — to reduce a hump while maintaining the natural continuity of the nasal ligaments and soft tissue. The result is a smoother, more natural-looking dorsum with less post-operative swelling, fewer grafts, and a lower risk of the over-operated appearance that can occur with traditional structural approaches.
Patients searching for preservation rhinoplasty in New Jersey will find that Dr. Rafizadeh's anatomic approach prioritizes structure, longevity, and natural proportion above all. The ideal candidate has a dorsal hump, good tip support, and skin that can accommodate the repositioned framework. Learn more about preservation rhinoplasty →
→ Preservation RhinoplastyPreservation rhinoplasty in New Jersey by Dr. Rafizadeh — push-down and let-down technique for natural dorsum reduction without removing cartilage.Open vs. Closed Rhinoplasty
The choice between open rhinoplasty and closed rhinoplasty is one of the most common questions patients ask before their consultation. In the open approach, a small incision across the columella gives Dr. Rafizadeh direct visibility into the entire nasal framework — ideal for complex reshaping, tip refinement, or revision cases where precision is critical. In the closed approach, all incisions remain inside the nostrils, leaving no external scar and reducing operating time and swelling for straightforward procedures.
Dr. Rafizadeh selects the approach based on each patient's anatomy and the complexity of the correction required — not personal preference or habit. Both open rhinoplasty in NJ and closed rhinoplasty in NJ are performed at his Morristown practice. Learn more about open vs. closed rhinoplasty →
→ Open vs. Closed RhinoplastyOpen vs closed rhinoplasty in New Jersey — Dr. Rafizadeh explains the difference, when each is used, and how the choice affects your result.Revision Rhinoplasty
Revision rhinoplasty — also called secondary rhinoplasty — corrects problems that persist or develop after a prior nose surgery. It is among the most technically demanding procedures in plastic surgery: scar tissue has disrupted normal anatomy, cartilage may have been over-resected, and familiar landmarks are altered. Dr. Rafizadeh is one of the few surgeons in the region with extensive experience in complex revision cases, and regularly sees patients from across New Jersey and New York City who are seeking a fix for a bad nose job in NJ.
Common revision concerns include a nose that appears pinched or over-reduced, a collapsed internal or external nasal valve causing breathing difficulty, residual humps or asymmetry, or a tip that has drooped or stiffened with time. Cartilage grafting — often harvested from the septum, ear, or rib — is frequently required to rebuild a stable framework. Learn more about revision rhinoplasty →
→ Revision RhinoplastySecondary nose surgery to correct over-reduction, asymmetry, collapsed valves, or an unsatisfying prior result.Ethnic Rhinoplasty
Ethnic rhinoplasty refers to rhinoplasty performed with explicit attention to preserving the patient's cultural identity and ethnic facial features. The goal is not to make every nose look the same, but to refine the specific concerns a patient has — a wide tip, a high dorsum, nostril asymmetry — while maintaining the characteristics that make their face recognizably theirs. Dr. Rafizadeh has extensive experience with Middle Eastern rhinoplasty in New Jersey, Persian rhinoplasty NJ, and rhinoplasty for patients of diverse backgrounds across the region.
Respecting ethnic anatomy is not a compromise — it is superior surgical judgment. Over-Westernized results that erase a patient's background are the most common cause of regret in rhinoplasty. Dr. Rafizadeh's goal is always a nose that fits the individual face, not a template. Learn more about ethnic rhinoplasty →
“The technique I choose is the one that best serves your anatomy and your goals — not the one I happen to prefer. Every nose is different, and the plan should be too.”
— Dr. Farhad Rafizadeh, MD FACS